
Recent guidelines suggest that both low- and high-risk patients can safely stop antibiotics when afebrile, clinically well and have completed an adequate treatment course, irrespective of neutrophil count in febrile neutropenia. This marks a departure from the usual practice of awaiting marrow recovery.
Category Archives: Tidbits
2025 M&M Year in Review
As 2025 concludes, we take a quick look back through our blog’s first year: the hits, the misses and what we have in store for 2026.
Furosemide: Flushing out the Misconceptions
Is it furosemide or frusemide? More importantly, what are its caveats and quirks? The evidence based is shockingly sparse for this ubiquitous medication…
Confessions of a “Penicillin Allergic” Patient
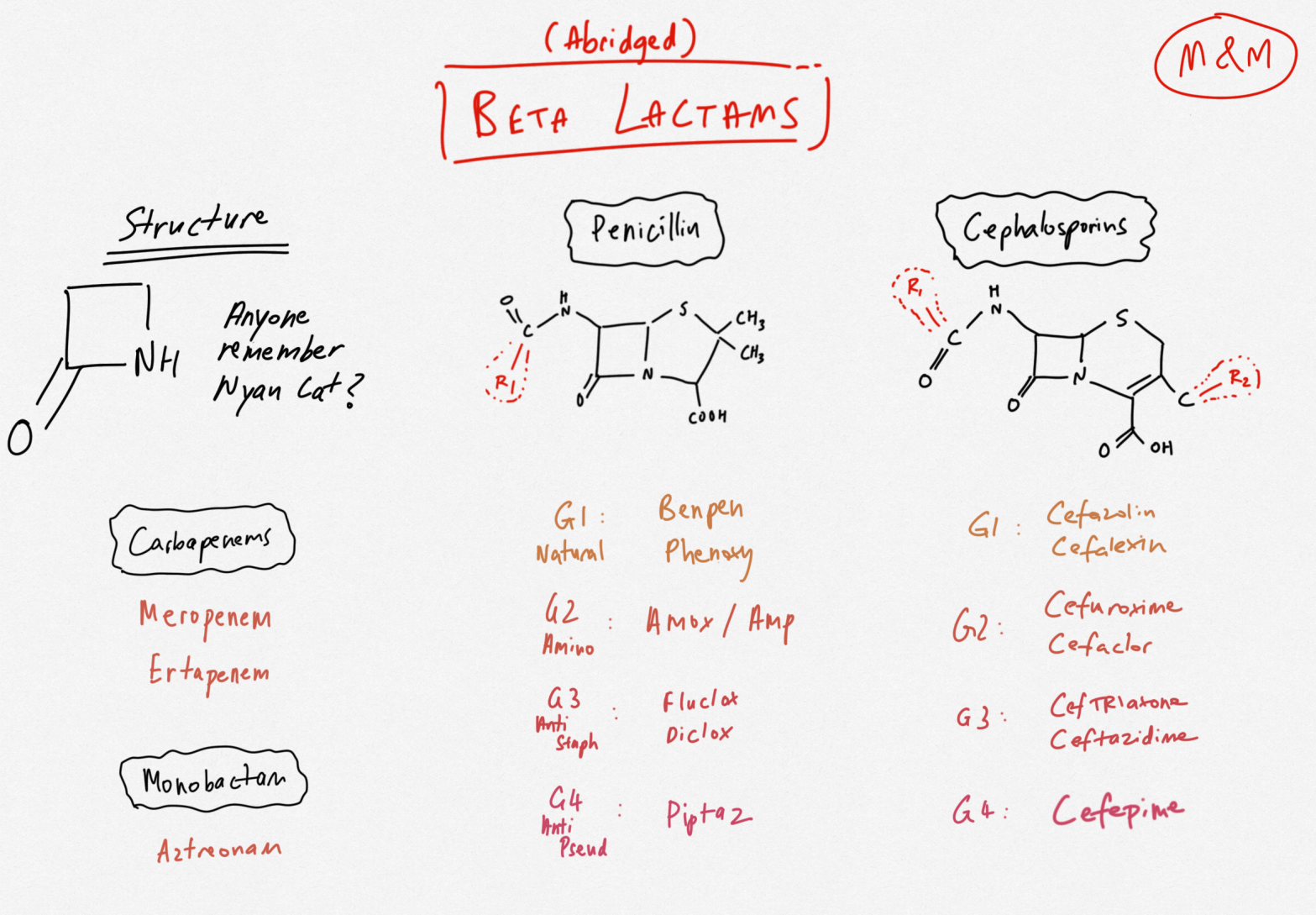
Penicillin allergies are exceptionally common – and exceptionally untrue. The oft quoted 10% cross-reactivity between penicillins and cefazolin is a relic of Penicillium past.
Learning Statistics – Against All Odds… or is it Risk?
Odds ratios and relative risk differ in their derivation and applicability, depending on study types. Hazard ratios are a different world of pain, and a time-dependent measure of rate. Even amongst published literature, these are incorrectly used interchangeably.
Sepsis: A Spoonful of Fluid Helps the Lactate Go Down

There are many more reasons than just hypoperfusion and anaerobic metabolism to explain the lactatemia in sepsis. It follows that there are many more considerations other than buckets of fluid when looking to lower the lactate.
The Fast and the Furious: Intravenous Fluid Shift

When administering urgent fluids, prioritize accessible options over central lines. Use larger and shorter cannulas for better flow rates, considering factors like the catheter’s gauge, length, and viscosity of the fluid. While central lines provide reliable access, they often hinder flow compared to suitable cannulas.
Stop trying to make Ammonia happen for hepatic encephalopathy in cirrhosis, it’s never going to happen.
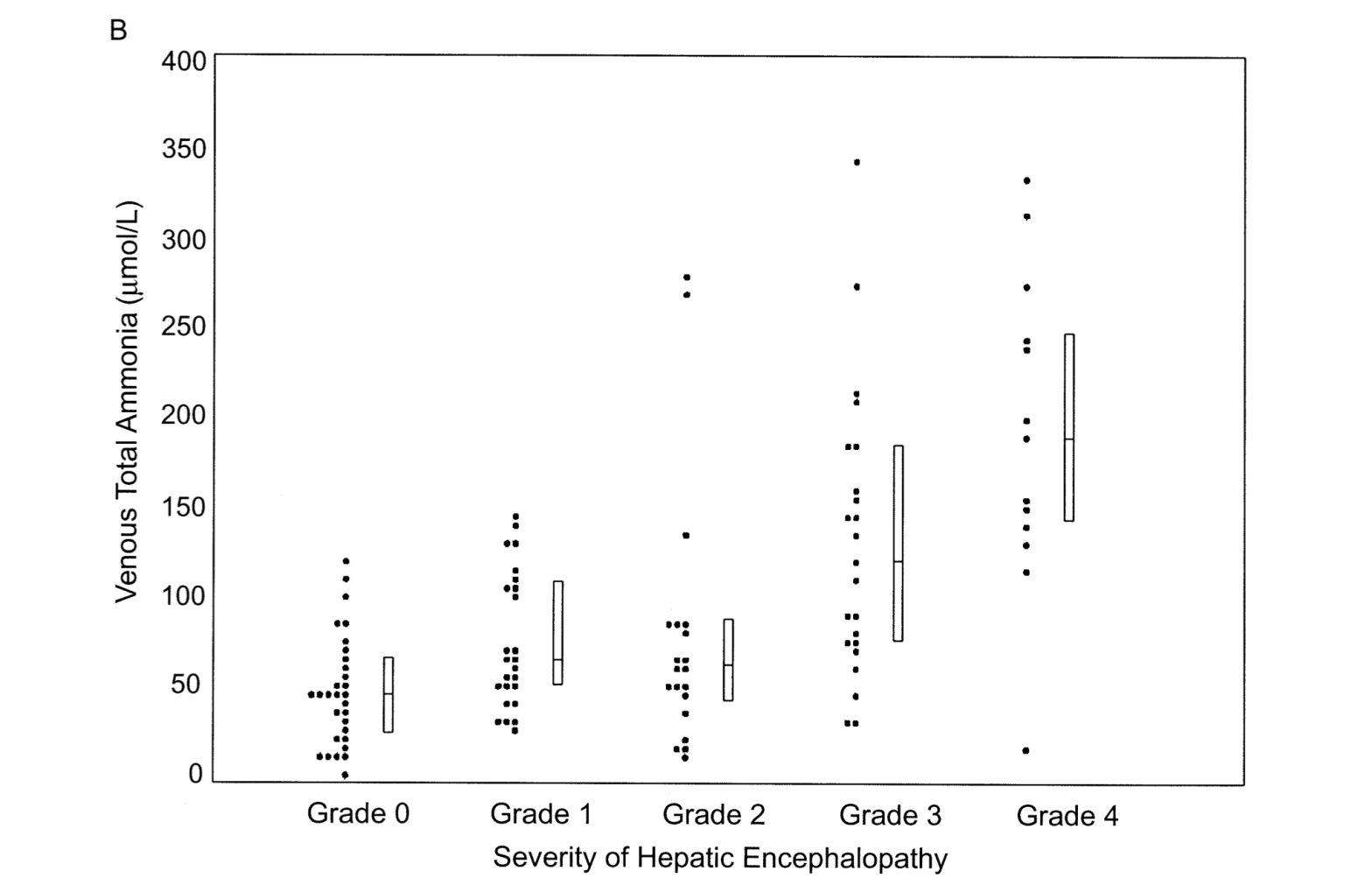
Ammonia’s importance in hepatic encephalopathy is hugely over-estimated. It cannot help to rule in, or rule out, a diagnosis of HE. Most unhelpfully, it is a really difficult test to collect, let alone interpret.
Meningitis: The Eternal Headache
Meningitis is exceedingly rare, but a clinically pertinent emergency laced with many a myth. Click to read more, but if this is happening, give antibiotics first.
(Not) Managing Asymptomatic Hypertension
Severe asymptomatic hypertension (BP > 180/110mmHg) in hospitalised patient is often mistakenly perceived as a call to antihypertensive action. Treat reversible causes, and consider a watch-and-wait approach. However, exceptions and caveats apply.
