Myth: Penicillin allergies. All of it.
Maladies:
1: Most ‘penicillin allergies’ are spurious – the majority can be safely de-labelled
2: Beta-lactam cross-reactivity is primarily determined by side chain similarity, not the shared ring structure
3: Cefazolin, and third generation cephalosporins and beyond (ie the ceftriaxone you overprescribe) often can be used in patients who have had a history of immediate penicillin hypersensitivity
4: Alternative antibiotics prescribed for “penicillin allergic” patients cause significantly worse outcomes
It has been a while, dear reader, however I was maimed. Though now in convalescence in a makeshift sanatorium, I shall use my affliction as the basis to educate the masses. You call it opportunistic, I say philanthropic.
Picture this. There I was, supine on the operating table, looking rather fetching in my surgical gown – I’ve not been neglecting my squats – pondering how on Earth one could miss three times on my wonderful veins, when I found myself in a far more perilous discussion. In my pre-anaesthetic enthusiasm, I attempted to educate the anaesthetist about the finer points of penicillin allergy. “Might we consider cefazolin?” I enquired with the casual confidence of someone who clearly hadn’t learned when to keep their mouth shut. His response was swift and unequivocal. My amoxicillin allergy qualified me for clindamycin, and I once again encountered the oft-cited 10% cross-reactivity between penicillins and cephalosporins, a relic from the era of jumpsuits and disco. As he easily put me on mute and started the sweet nectar I’ve become accustomed to, I resolved to set the record straight for my tens of loyal readers.
Before I begin, I would like to clarify some terms. The following is only going to discuss penicillin allergy. An allergy is an IgE-mediated reaction (aka type I hypersensitivity reaction). For those of you who roll your eyes at the mention of immunoglobulins, an allergic reaction is an acute illness occurring after exposure to an allergen – think generalised urticaria, pruritus, angioedema, abdominal pain, wheeze, airway compromise etc. Anaphylaxis is a severe allergic reaction, with the general definition being involvement of at least two systems, for example skin/mucosal and respiratory. However, antibiotics can also cause other types of hypersensitivity reactions, such as severe cutaneous adverse reactions (SCAR), including SJS, TEN, DRESS (type IV hypersensitivity). I will not discuss these here, but will say that the following does not apply to those cases. If your patient has a documented history of SCAR, call Immunology if they need antibiotics.
The Scarlet Letter
Or in this case, that scarlet ID band. Around 10-15% of people report a penicillin allergy, however, when formally tested < 1% of this cohort will have a true allergy – and even fewer will have a serious allergy [1]. The remaining carry a label granted as a result of childhood exanthemata, ones which you will never be able to get a proper history on. In other cases, there may be non-specific symptoms that patients confuse for an allergy – such as blurry vision, or isolated gastrointestinal upset.
The label of penicillin allergy is not trivial. Patients with a penicillin allergy label naturally receive broad-spectrum antibiotics, which also come with the promise of C. difficile infection, MRSA and VRE, increases in surgical site infections, nephrotoxicity, and even an increase in mortality. Then there’s all the stats that medical administrators will gush over, with longer hospital stays, higher readmission rates, and increasing the economic burden on the healthcare system [2].
The Molecular Mechanics of Mischief
The mythical 10% rate stems from studies in the 1960s and ‘70s, when cephalosporins were manufactured using the same Penicillium fungi as penicillins, likely leading to contamination [3]. Since artificial production became standardised in the mid-1980s, these contamination issues vanished faster than my dignity in that operating theatre.
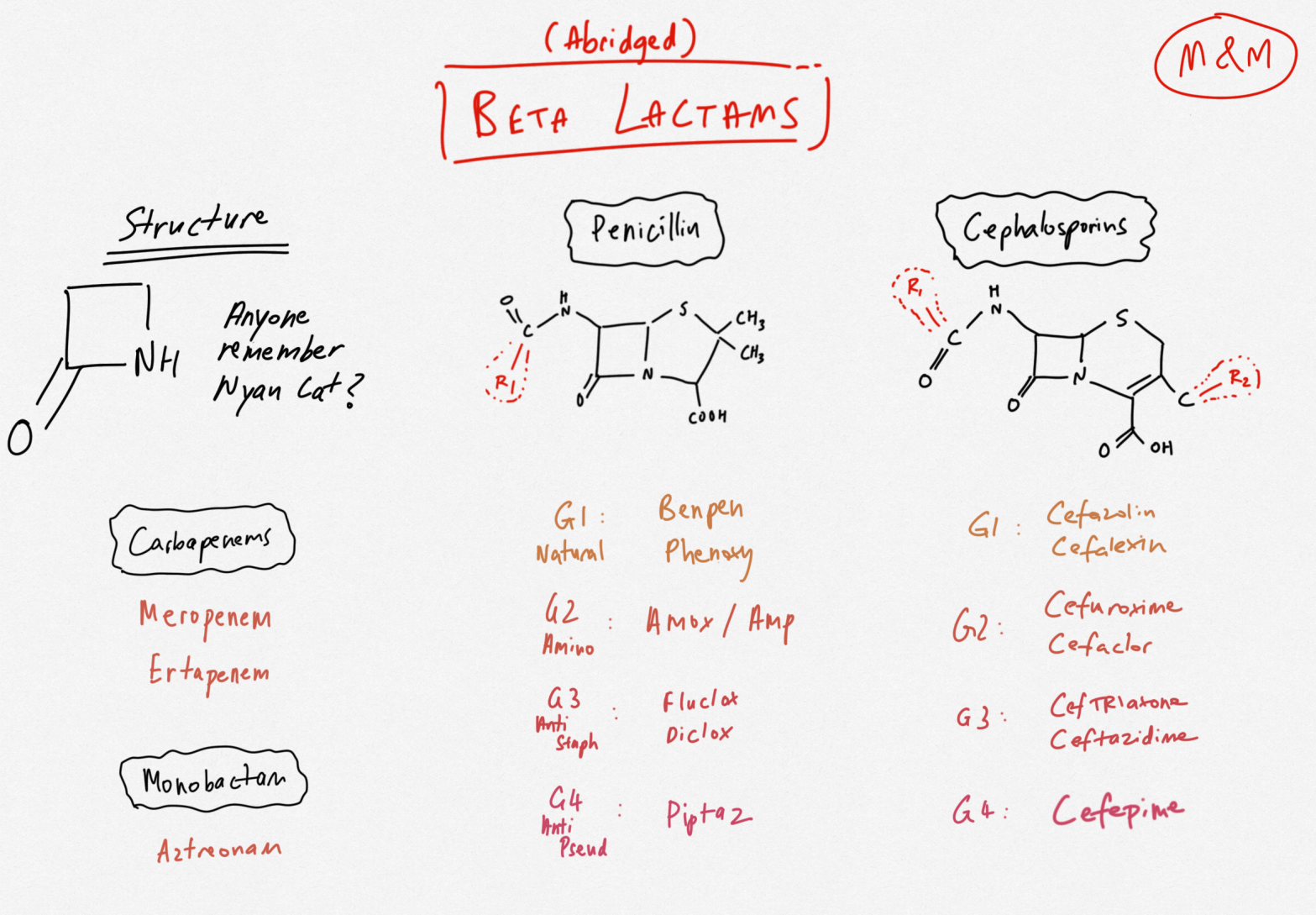
To understand why this is such spectacular nonsense, we must delve into some basic immunology and pharmacology. For a molecule to provoke an IgE-mediated allergic reaction, it must do more than simply exist. Beta-lactam antibiotics, which, for the sake of simplicity can be categorised into penicillins, cephalosporins, carbapenems, and monobactams – beautifully illustrated here by our in-house colourblind illustrator:
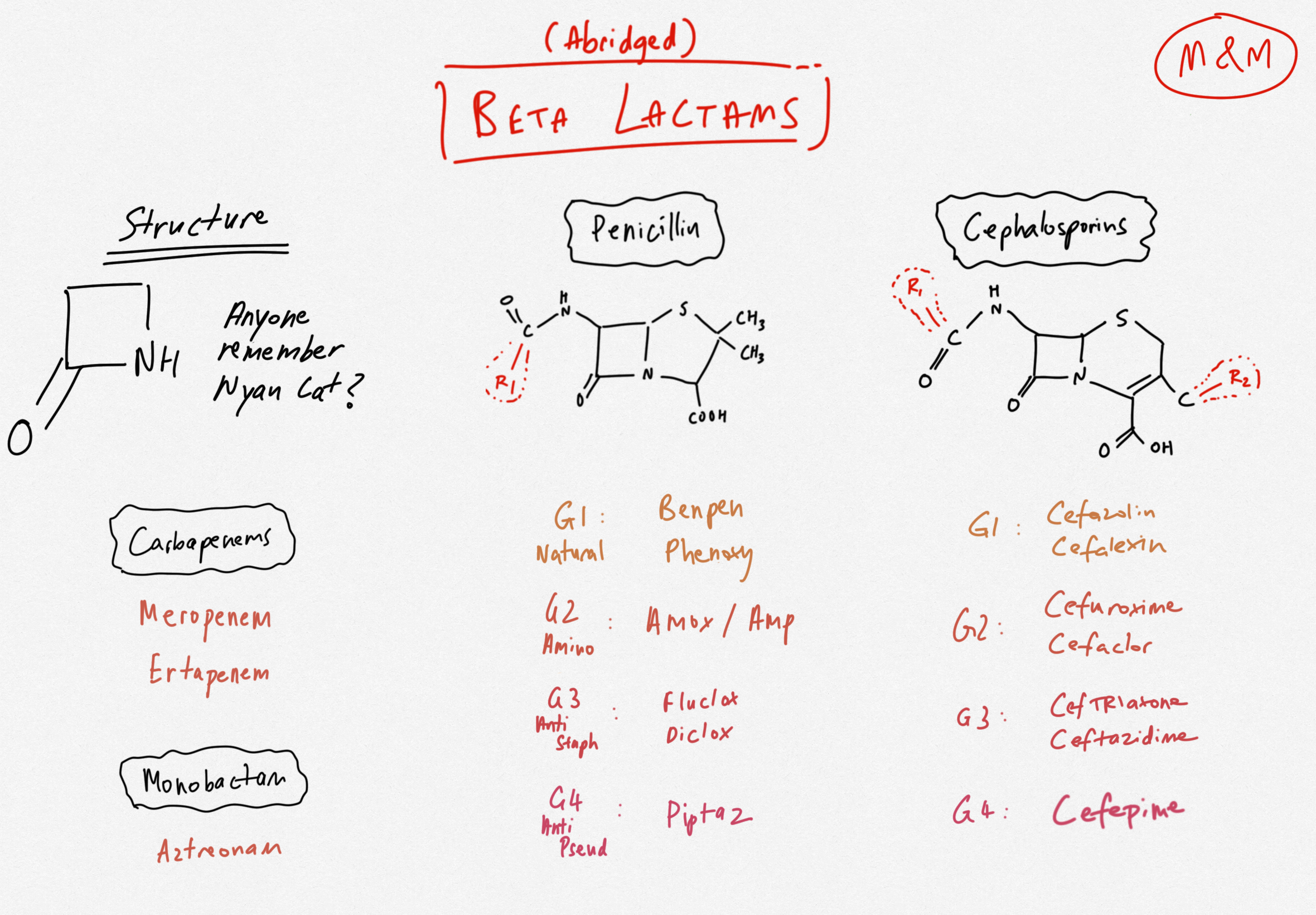
When metabolised, their molecules are broken down. On their own, these are all too small to raise an antibody army by themselves. They instead act as haptens, molecules which become immunogenic only when covalently bound to host proteins. The immune system can then bind this hapten-protein complex and IgE is eventually formed against them [4]. This, by the way, is also why it is impossible to mount an IgE-mediated reaction to iron infusions – elemental iron atoms cannot form covalent bonds, and therefore can’t invite IgE to the party. More on that in another article.
All beta-lactams share a four-membered ring that you have all heard of. They each however have additional decorative rings which distinguish the classes. Without boring you any further, I will get to the plot twist. The shared beta lactam ring is about as relevant to cross-reactivity as the model of your Littmann is to your ability to hear murmurs. In fact, the beta lactam ring is very rarely the cause of allergy [3].
Cross-reactivity is primarily determined by similarity of side chains (and mainly the R1 chain. My top fashion rule also applies here: accessories make the outfit. There is a fantastic EMCrit article on this which explores the structural cross-reactivity in great detail, however the one to remember for Australian practice (see eTG) would be the potential for cross-reactivity between aminopenicillins (e.g. amoxicillin and ampicillin) and cephalexin.
Cefazolin, on the other hand, the love of which is my only common-ground with my orthopaedic colleagues, has a unique side-chain profile which does not share any similarity with other beta-lactams. In saying this, as it is the most commonly used perioperative prophylactic antibiotic, the incidence of perioperative cefazolin allergy has been increasing (though is still rare enough). Based on what we know about the side chain profile however, we could still trial a penicillin or another cephalosporin in a patient with a cefazolin allergy. Echoing this is the recent changes in the eTG which now recommend giving cephalosporins for hospitalised patients who even have a history of anaphylaxis to penicillins (see topic ‘Penicillin Hypersensitivity’ under Antibiotic for another great resource).
Carbapenems basically have non-existent R1 side-chains, and they are also notoriously non-reactive. The rate of cross-reactivity in those with penicillin allergy was 0.3% in one study [5]. Guidelines also state that they can be given to those with documented penicillin allergy without any allergy testing (see eTG and ASCIA guidelines below). The case of carbapenems even has become an argument for why it is possible that most of the immunogenicity of beta-lactams comes from their side chains, and not the ring itself.
A quick note on Australia’s favourite antibiotic, tazocin. Tazocin allergy itself is rather rare (except in patients with cystic fibrosis, likely due to overexposure) [6]. It also bears no resemblance to the other penicillins, and therefore the expected cross-reactivity would be low. Patients can however be allergic to both, or even to the beta-lactamase component (tazobactam). Either way, a documented history of penicillin allergy is not an absolute contraindication to using tazocin, but I understand why your indemnity provider may think otherwise.
Practical Tips to Contribute to the Delabelling Revolution
There are so many great resources on this, some of which are linked below, however here is my two-cents:
1. Take a careful history. Determine timing, symptoms and treatment. Use the PEN-FAST tool. Many patients who have had anaphylaxis will be able to tolerate penicillins after 10 years.
2. De-label the allergy. When a patient tolerates penicillin or a cephalosporin, update the medical record. De-labelling decreases morbidity, antibiotic resistance and costs.
3. Avoid broad-spectrum substitutes unless necessary. Vancomycin and clindamycin are not the solution. Use them only if the patient has had a confirmed, severe and recent beta lactam allergy (or delayed non-IgE-mediated reactions such as severe cutaneous adverse reactions which we have not mentioned in this article).
4. Consider a beta-lactam with low likelihood of cross-reactivity – consult Immunology for advice, and whether sensitivity testing is required.
Giant’s Shoulders:
EMCrit re: Pencillin allergies. Excruciating detail.
eTG topic on ‘Penicillin Hypersensitivity’ and ‘Principles of assessing patients reporting antimicrobial hypersensitivity’
ASCIA statement on Penicillin allergy
Also Cited Above:
[1] Devchand M and Trubiano JA with a practical approach to assessment and prescribing.
[2] Recent systematic review by Zhang et al.
[3] Excellent review by Pichichero et al – recommended further reading
[4] Hapten concept in beta-lactam allergy
[5] A review about carbapenem allergy by Lee and Bradley
[6] A study of piptaz allergy across European allergy centres
Discover more from Myths & Maladies
Subscribe to get the latest posts sent to your email.

1 Comment
Comments are closed.